The value of sensitivity in both the atrium and the ventricle can be set at a fixed value or can be programmed on Autosensing. Autosensing is different than the adaptive sensitivity used in implantable defibrillators.
Autosensing
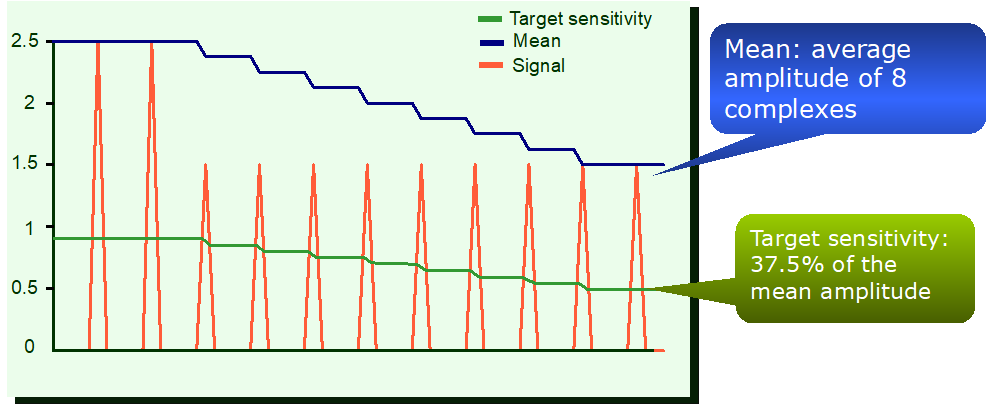
The atrial and ventricular sensed signals are permanently monitored. The amplitude of the signals is averaged over rolling windows of 8 cycles.
- average of the 8 previous complexes
- automatic adaptation of the sensitivity threshold in both cavities
- sensitivity automatically programmed at approximately 1/3 of the averaged amplitude
Atrial Autosensing
A bipolar atrial lead is required for atrial Autosensing.
- following a premature atrial contraction (atrial detection in the WARAD), the device enters in AA suspicion phase and the atrial sensitivity is immediately set to 0.4 mV to optimize atrial sensing (onset of an atrial arrhythmia with low amplitude signals)
- if the premature atrial contraction is isolated the atrial sensitivity is progressively adjusted to the reference value
- atrial sensitivity is also forced to 0.4 mV, when the atrium is paced and during Fallback mode
Ventricular Autosensing
- the ventricular sensitivity is forced to 1.5 mV (bipolar configuration) or to 2.0 mV (unipolar configuration) when the ventricle is paced
- the values of 1.5 mV (bipolar) and 2.0 mV (unipolar) are not programmable