Patient
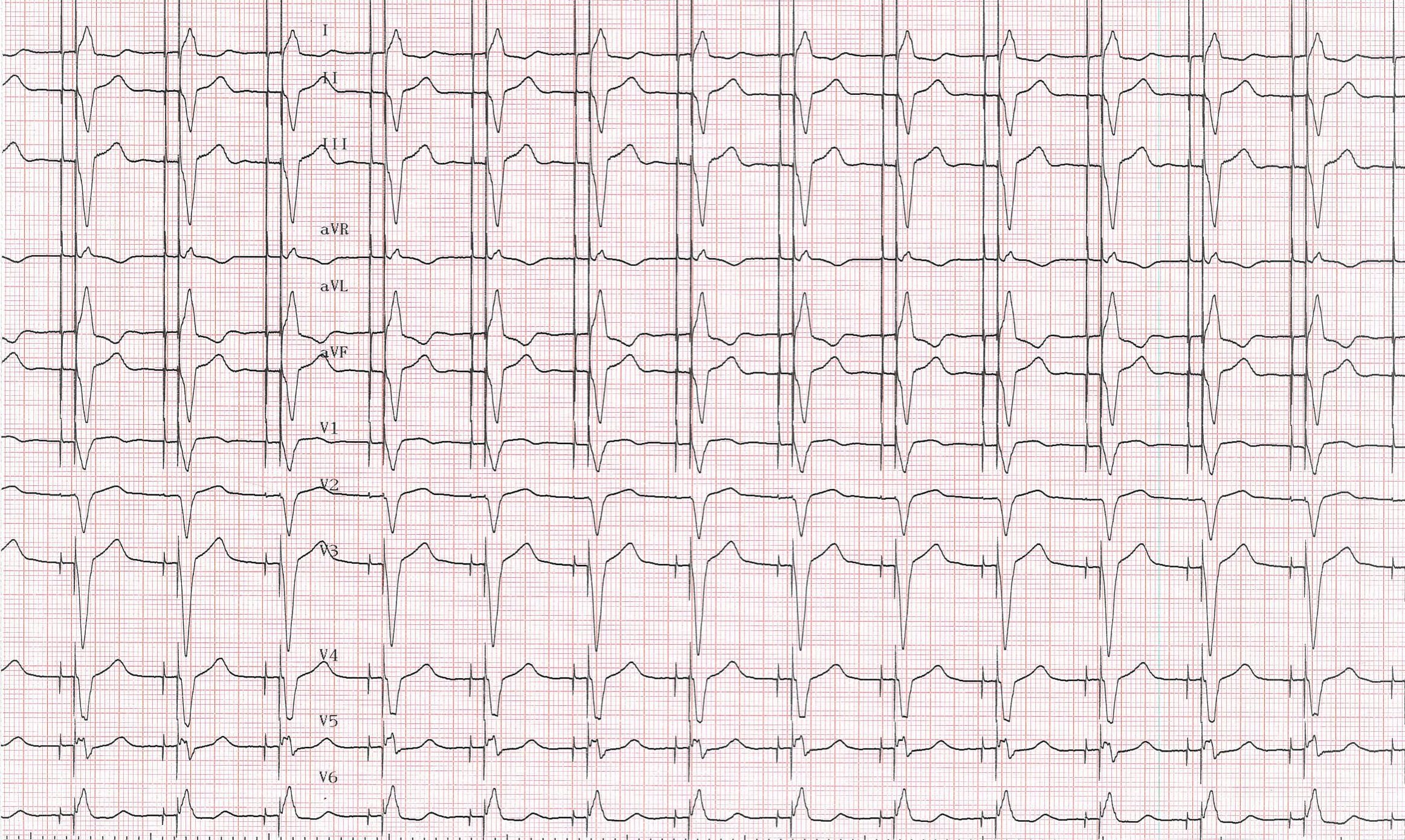
- 78-year-old man
- syncope and complete atrio-ventricular block
- Advisa DR MRI (Medtronic) dual-chamber pacemaker
- right atrial lead at the appendage, right ventricular lead at the apex
- 2 days after implantation, pacemaker control
Master MicroPort CRM!