MRI: why do we take precautions?
Magnetic resonance imaging (MRI) is one of the most powerful diagnostic tools available in modern medicine. It provides unmatched tissue detail, no radiation exposure, and is indispensable in cardiology, oncology, neurology, and orthopedics. Today, most pacemaker and ICD patients can safely undergo MRI — yet every scan must follow a clear safety protocol. Understanding why precautions are taken, and how they differ between manufacturers and device types, is essential for every allied professional involved in patient care.
1. Why precautions are necessary
In older (“non-MR-conditional”) cardiac devices, these fields could theoretically:
-
Activate a reed switch or reset the device,
-
Cause oversensing or pacing inhibition,
-
Induce currents in leads (risking myocardial heating),
-
Temporarily affect sensing or battery voltage.
Modern devices are engineered to withstand these effects. They use non-ferromagnetic materials, improved filtering, and “MRI mode” programming to prevent inappropriate pacing or shocks. Still, precautionary checks are essential before, during, and after every scan.
2. General principles for MRI with pacemakers and ICDs
Before MRI
-
Confirm the system (device + leads) is MR-conditional and has no abandoned or fractured leads.
-
Wait at least six weeks after implantation, unless the scan is clinically urgent and approved by the cardiologist.
-
Ensure normal lead thresholds, impedances and device battery life.
-
Program the device into MRI mode — or equivalent asynchronous pacing for non-conditional systems.
During MRI
-
Monitor ECG and pulse oximetry continuously.
-
Ensure immediate access to a programmer, external defibrillator, and trained staff.
After MRI
-
Restore normal settings, check lead measurements, and confirm rhythm stability. This is not applicable to MicroPort devices, if all the conditions for an MRI examination have been met and the «MRI mode» has been activated, either in «AUTO» or in «Manual» mode.
-
Review the remote monitoring transmission if automatically generated.
3. Pacemaker vs. ICD: key differences
| Aspect | Pacemaker (PM) | Implantable Cardioverter-Defibrillator (ICD) |
|---|---|---|
| MRI mode | Usually switches to asynchronous pacing (AOO/VOO/DOO) | Tachyarrhythmia detection and therapies disabled |
| Timeout option | Auto-exit after 12–48 h depending on manufacturer | Usually shorter (3–9 h) for safety |
| Risk if left in MRI mode | Minor (asynchronous pacing) | Medium for MicroPort ICDs — no shock therapy if an arrhythmia occurs only during MRI exam (during monitoring period the arrhythmia detection and therapies are activate). |
| Post-scan step | Device check or automatic reversion | Immediate verification required; confirm shocks are re-enabled
or automatic reversion for MicroPort ICDs |
4. Vendor-specific precautions and workflows
MicroPort
-
All MR-conditional MicroPort devices (Kora, Alizea, TEO, ENO, OTO) include the AutoMRI™ sensor.
-
Once activated (up to 10 days before the scan), AutoMRI™ automatically detects the MRI magnetic field and switches to the programmed asynchronous mode.
-
It returns to normal settings automatically about 5 minutes after leaving the scanner.
-
If remote monitoring is active, a post-MRI alert is automatically sent.
-
Workflow: Activate AutoMRI™ a few days before the exam → perform MRI → confirm automatic reversion via remote transmission.
-
Verify the MRI compatibility of implanted MicroPort CRM device with the dedicated website: https://www.crm.microport.com/automri/en/cardiologist
-
Read the MRI Solution manual associated with the PM/leads or ICD/leads system (https://www.microportmanuals.com/library3.php?z=EU&lib=MRI%20Solutions&l=1&th=crm). It is an addendum to the implant manuals and provides important information about conditions for use and contraindications of examination using MRI of patients implanted with a PM or ICD system. It is designed for cardiologists, physiologists or other healthcare professionals programming PM or ICD, as well as for radiologists, technologists or other healthcare professionals performing the MRI examination.
-
MR-conditional MicroPort ICDs (ULYS, EDIS, GALI, TALENTIA, ENERGYA) include the AutoMRI™ sensor .The AutoMRI™ feature automatically detects the MR field and automatically switches into asynchronous MRI mode (especially OOO) and deactivates essential therapies (atp + shock). After the MRI scan, the device switches back to its initial settings without any HCP intervention.
For non-MR-conditional MicroPort systems:
Program manually to asynchronous pacing (AOO/VOO) at least 20 bpm above intrinsic rhythm; disable capture management and magnet response.
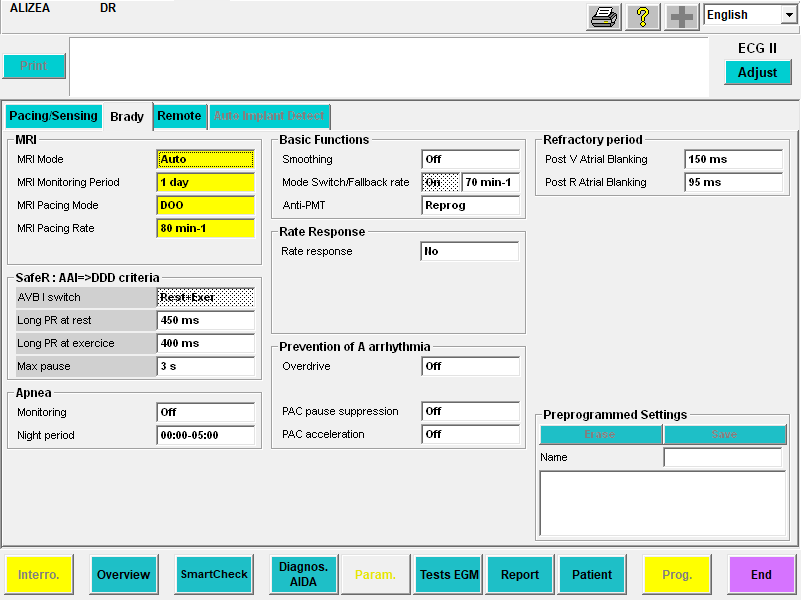
Below are screenshots of PM and ICDs MicroPort with Auto MRI mode set to Auto:
Alizea DR
GALI 4LV SonR CRT-D

Medtronic
-
MRI-safe mode: SureScan™.
-
For most models, activation/deactivation is manual.
-
High-voltage devices (ICD/CRT-D) include a 6-hour automatic timeout; Azure™ and Micra™ pacemakers have a 24-hour timeout.
-
MRI can also be controlled directly by radiology via CareLink SmartSync™ MRI Access, allowing automatic pre-scan checks and programming.
-
Post-MRI verification is required in person or through remote monitoring.
-
Non-conditional systems can often be scanned safely at 1.5 T with proper supervision.
Biotronik
-
Uses MRI AutoDetect and the newer MRI Guard 24/7 in Amvia models.
-
When activated, the device automatically switches to MRI mode upon entering the magnetic field and reverts instantly afterward.
-
MRI Guard 24/7 means the MRI sensor is permanently active, eliminating the need to program before each scan.
-
If home monitoring is active, an automatic transmission confirms proper exit from MRI mode.
Abbott
-
MRI mode must be activated before scanning and deactivated afterward.
-
Timeout feature (3–12 h) automatically exits MRI mode for ICDs.
-
Recent devices support Remote Support through Merlin™ 2 programmers — enabling remote activation and deactivation of MRI settings in authorized centers.
-
Always verify SAR and B1+rms parameters are within device limits.
Boston Scientific
-
MRI mode: ImageReady™.
-
Requires pre- and post-scan activation, with programmable timeout (12–48 h for pacemakers, 3–12 h for ICDs).
-
Radiology must confirm scanner conditions (field ≤ 1.5 T or 3 T depending on system, slew rate, SAR ≤ 2 W/kg).
-
Remote programming can be assisted by HeartConnect™, a secure online link between radiology and a remote programmer.
5. Patients with non-MR-conditional or legacy systems
Large studies now show that MRI at 1.5 T can be safe even in patients with older devices, provided there are no abandoned or epicardial leads, and the generator is pectoral (not abdominal).
-
The device is programmed to a simple, stable pacing mode (AOO/VOO/DOO or ODO/OVO),
-
Tachy detection is turned off,
-
Patients are monitored continuously, and
-
Immediate post-scan interrogation is performed.
Rare risks—such as power-on reset or small changes in sensing thresholds—occur in <1% of cases.
Abandoned and epicardial leads remain a grey zone; these patients should be scanned only in specialized centers with cardiology supervision and advanced monitoring.
6. Role of remote monitoring
Remote monitoring ensures patient safety after the MRI:
-
Detects whether the device correctly reverted from MRI mode.
-
Reports lead parameters, sensing, and battery status.
-
Alerts staff in case of device reset, lead noise, or inappropriate therapy inhibition.
Allied professionals should confirm the transmitter or app is connected before the scan and advise patients to keep it near them for the following 24–48 hours.
7. Key messages for practice
-
Most CIED patients can safely undergo MRI.
MR-conditional labeling means the combination of device + leads + scan conditions was tested and certified safe. -
Even non-conditional systems may be scanned if risk is justified and proper precautions are taken.
-
Do not scan within the first 6 weeks after implantation, unless cleared by the cardiologist.
-
Abandoned or epicardial leads require individualized assessment.
-
Always verify MRI mode activation and post-scan deactivation or timeout.
-
Remote monitoring is your ally—confirm connectivity before and after MRI.
8. What to tell patients
-
“Your pacemaker/ICD can safely go through MRI if programmed correctly.”
-
“It’s normal for your heartbeat to feel a little faster during the scan.”
-
“Your remote monitor will tell us when the scan is done.”
-
“Avoid scheduling MRI in the first few weeks after your implant.”
Conclusion
Thanks to rapid technological evolution — especially automatic MRI detection, timeout safety features, and remote monitoring— MRI has become safe for nearly all pacemaker and ICD patients.
Allied professionals play a vital role: confirming patient identity, preparing the device, maintaining communication with radiology, and verifying recovery afterward.
With these steps, MRI is not only possible — it is routine, efficient, and safe.