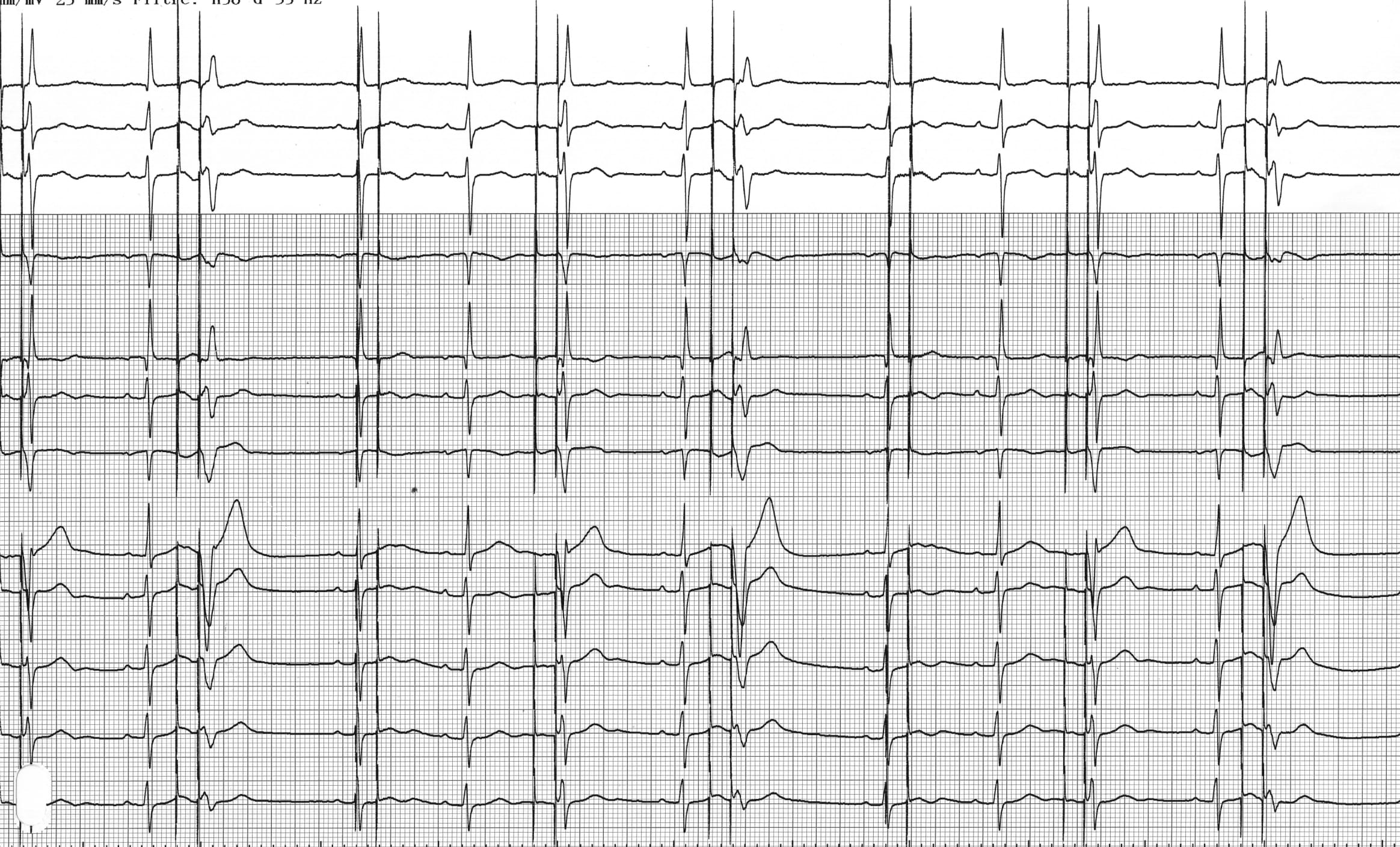
Patient: 69-year-old man implanted with a Medtronic dual-chamber pacemaker following repeated syncopes due to sinus node dysfunction; the 2 pacing leads are well positioned with normal pacing impedances, correct sensing and satisfactory pacing thresholds; 3 days after implantation, pacemaker evaluation; programming of various pacing modes and recording of tracings; for this first tracing, ; device programmed to DOO mode;
Case Summary
0 of 1 Questions completed
Questions:
Information
You have already completed the case before. Hence you can not start it again.
Case is loading…
You must sign in or sign up to start the case.
You must first complete the following:
Results
Results
0 of 1 Questions answered correctly
Time has elapsed
Categories
- Not categorized 0%
-
DOO mode
ECG 2A: On this tracing, there is regular atrial and ventricular pacing at a rate of 40 bpm; atrial and ventricular capture is effective only when it occurs outside the myocardial (atrial and ventricular) refractory periods; this pacing is asynchronous, atrial and ventricular activities are not sensed and therefore cannot inhibit pacing; when ventricular pacing occurs at the peak of the T wave, there is capture with an arrhythmogenic risk;

ECG 2B: The EGMs show that the atrial and ventricular signals are tall but not sensed (mode DOO) explaining the asynchronous pacing;
Comments: The DOO operating mode is reversed compared to the ODO mode: no sensing is possible and pacing is at fixed intervals. Asynchronous modes at fixed rate were the only modes available on the first pacemakers. The DOO mode induces asynchronous sequential atrioventricular pacing, without inhibition by intrinsic events. As seen on this tracing, when the patient is not device-dependent, parasystole occurs with competition between spontaneous activities and paced activities. This mode allows to verify the effectiveness of the pacing and to avoid inhibition in case of exposure to an external interference (electric scalpel in a dependent patient, for example). Pacing is effective and captures the atrium or ventricle only when it occurs outside the absolute physiological refractory period following a spontaneous atrium or ventricle.
This tracing shows the risk of this type of mode. Several ventricular pacings occur at the peak of the T wave of an unsensed spontaneous QRS. This is the vulnerable period with risk of induction of a ventricular rhythm disorder. The risk of ventricular fibrillation is limited although increases in the presence of myocardial ischemia or metabolic disorder. Similarly, asynchronous atrial pacing in an atrial vulnerable period can induce atrial fibrillation.
Asynchronous modes are now obsolete and are only used in 2 specific circumstances: 1) in a magnetic mode or magnet mode; indeed, the application of a magnet causing AOO, VOO or DOO pacing depending on the programmed mode, 2) the DOO mode can be programmed temporarily in dependent patients with an MRI-compatible pacemaker who need to undergo an MRI.
Take-home message: Pacing in a ventricular or atrial vulnerable period can be arrhythmogenic and favor the occurrence of a ventricular or atrial arrhythmia which is most often polymorphic;
- 1
- Current
- Review
- Answered
- Correct
- Incorrect
-
Question 1 of 1
1. Question
Regarding this ECG, which answer(s) is(are) true?
CorrectIncorrect