Patient
- 83-year-old man
- atrial fibrillation and complete atrio-ventricular block
- implantation of a Micra leadless pacemaker (Medtronic)
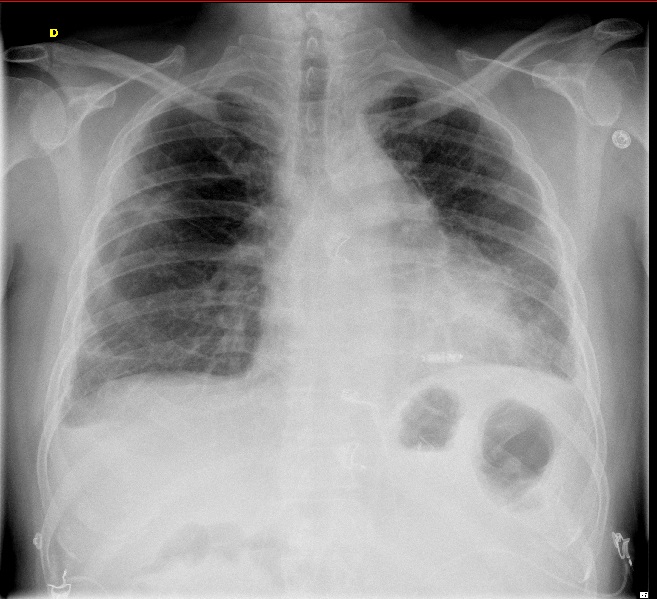
Chest X-ray: antero-posterior view
- leadless pacemaker (linear radiopaque device) in the septo-apical region
leadless pacemaker
Case Summary
0 of 1 Questions completed
Questions:
Information
You have already completed the case before. Hence you can not start it again.
Case is loading…
You must sign in or sign up to start the case.
You must first complete the following:
Results
Results
0 of 1 Questions answered correctly
Time has elapsed
Categories
- Not categorized 0%
-
Comments
- since the first cardiac pacemaker was implanted in 1958, pacing technology has seen iterative changes resulting in improved battery life, lead performance, miniaturization and device programming; however, the basic design of cardiac pacemakers has remained relatively unchanged: a pectoral pulse generator connected to 1 or more transvenous leads
- although highly reliable, conventional cardiac pacemakers have several limitations; the subcutaneous position of the generator predisposes to local complications such as skin erosion, pocket hematomas and infection; insertion of transvenous leads can result in acute complications, such as pneumothorax or dislodgement; presence of chronic transvenous leads can lead to central vein obstruction, tricuspid valve insufficiency, endocarditis or conductor fracture
- in the last decade, several technological advancements mainly in catheter-based delivery systems, miniaturization, high-density energy source, lowered energy consumption and novel communication technologies, have allowed the development of a leadless standalone system with a totally self-contained intracardiac pacemaker
- leadless pacemaker represents a disruptive technology which may revolutionize the field of cardiac pacing
- two leadless pacing systems are currently clinically available: the Nanostim Leadless Cardiac Pacemaker (LCP, Abbott), and the Micra Transcatheter Pacing System (TPS, Medtronic); both are fully self-contained units capable of providing single-chamber right ventricular pacing
- the Nanostim is longer (42 mm versus 25.9 mm), the Micra wider resulting in moreless similar volumes
- the implant procedure for both systems is similar, utilizing a percutaneous femoral, catheter-based approach to introduce and advance the leadless pacemaker to the right ventricle (RV)
- main differences between the systems are related to the fixation; the primary fixation mechanism of the LCP device is a screw-in helix with a maximum penetration depth in tissue of 1.3 mm; three nylon tines provide a secondary fixation mechanism by avoiding unscrewing of the helix; the fixation mechanism of the TPS comprises four flexible self-expanding nitinol tines
- severe complications, including cardiac perforation, tamponade and deaths have been described in a limited number of patients
- another significant limitation of these devices is the restriction to single-chamber ventricular pacing
- because only 10%-20% of current transvenous implants are single-chamber devices, the potential clinical use of LCPs may be restricted to chronic atrial fibrillation with slow ventricular response; however, current guidelines for single-chamber pacing also recommend consideration in patients with complete AV block who are elderly and have a low activity level, and patients with sinus node dysfunction and infrequent pauses; leadless pacemaker also offers an option for patients with difficult venous anatomy and for patients who are not candidates for transvenous systems
To expand the indications of leadless pacing to more patients, efforts are being made to develop multicomponent, communicating leadless systems capable of performing dual-chamber pacing and cardiac resynchronization therapy; challenges for development of dual-chamber and cardiac resynchronization leadless pacing stem from the need for interdevice communication, minimization of interference, ability to interrogate simultaneous devices, and the likely need for a device large enough to accommodate the required circuitry without significantly impacting battery life.
- 1
- Current
- Review / Skip
- Answered
- Correct
- Incorrect
-
Question 1 of 1
1. Question
The atrial fibrillation of this patient is probably
CorrectIncorrectHint
Nothing to do with the X-ray!