Sinus node disease
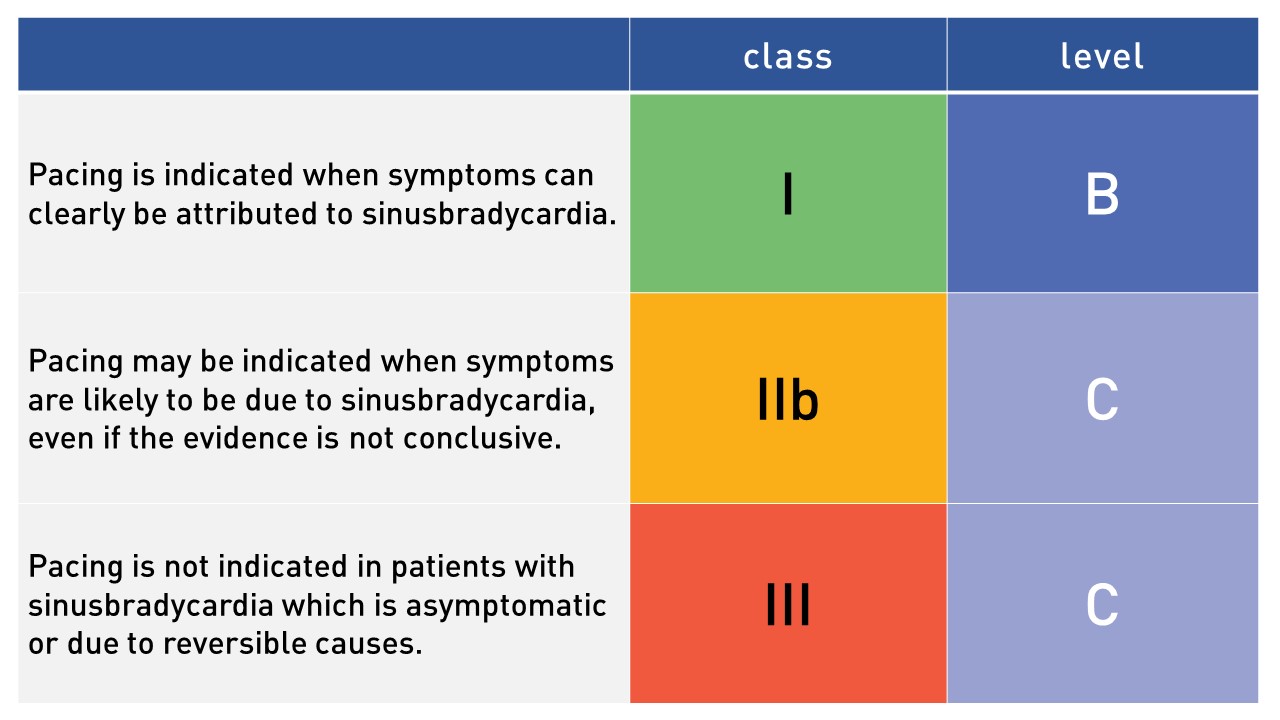
There is a strong consensus that patients with symptomatic sinus node disease will benefit from cardiac pacing for symptom relief (class 1 recommendation with level of evidence B). Demonstrating a clear cause–effect relationship between symptoms and sinus node disease is often difficult to achieve. When the evidence is non-conclusive, the ESC warrants a IIb – C recommendation for pacemaker implantation. Asymptomatic sinusbradycardia or sinusbradycardia causes by reversible causes is no indication for implantation (III C).
Table adjusted from the ESC guideline for sinus bradycardia:
AV conduction disease
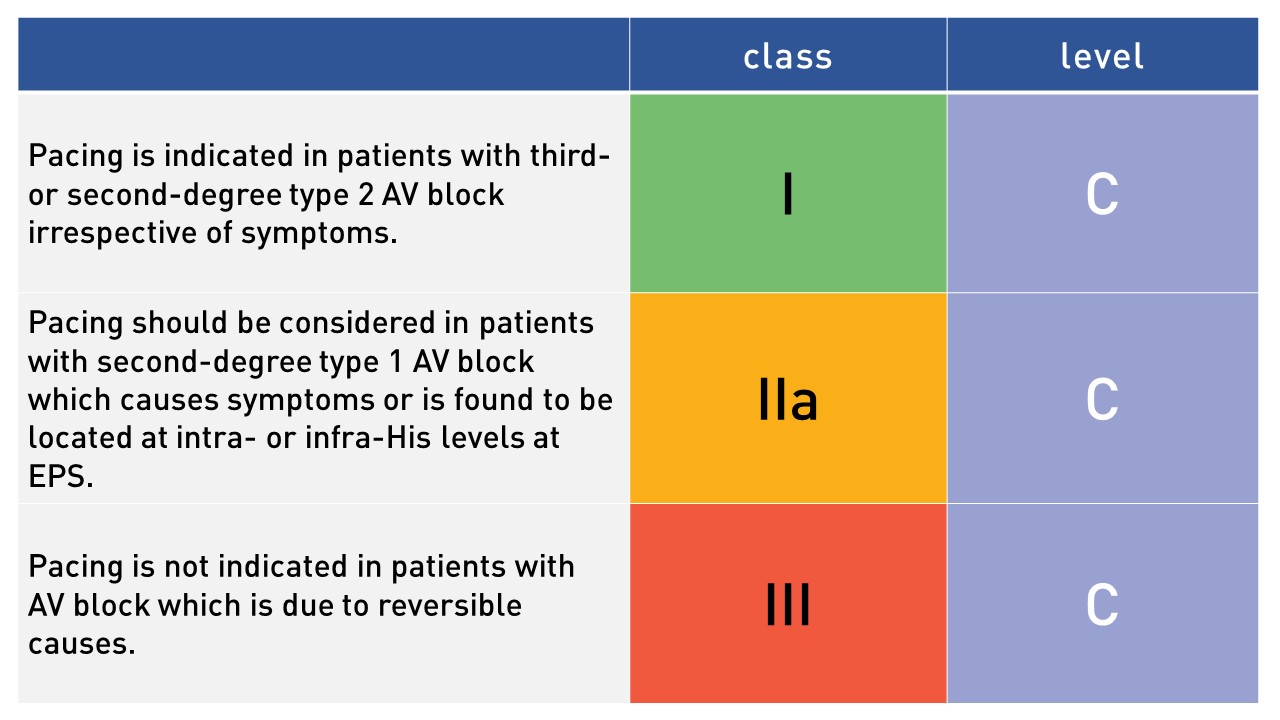
There is also strong consensus that permanent cardiac pacing is indicated in patients with third- or second degree type 2 AV block, regardless of symptoms (I C recommendation). In patients with type I second-degree AV block, the decision about pacing is controversial, taking into account the severity of symptoms and the risk of progression to complete AV block. In patients with second-degree type 1 AV block which causes symptoms or is found to be located at intra- or infra-His levels at electrophysiological study, pacemaker implantations should be considered (IIa C recommendation).
Table adjusted from the ESC guideline for AV block:
Choice of pacemaker
When the decision to implant a pacemaker has been made, the type of pacemaker needs to be considered: with atrial lead, ventricular lead or both. Dual-chamber pacemaker is advised for patients with AV-blok and also for patients with sick sinus node disease since it is associated with less occurrence of atrial fibrillation, stroke and pacemaker syndrome as compared with single-chamber pacemakers. In case of permanent atrial fibrillation and AV-block, a single-chamber pacemaker in VVI(R) mode may suffice. In patients with left ventricular systolic dysfunction and ventricular conduction delay (left bundle branch block or QRS of at least 150 ms) or in whom it is expected that the right ventricle will receive a lot of pacing, the addition of a left ventricular lead to enable cardiac resynchronization therapy (CRT) is indicated.