Anodal capture
Case Summary
0 of 1 Questions completed
Questions:
Information
You have already completed the case before. Hence you can not start it again.
Case is loading…
You must sign in or sign up to start the case.
You must first complete the following:
Results
Results
Time has elapsed
Catégories
- Pas classé 0%
-
An abrupt change on an impedance trend should rise the suspicion of lead dysfunction. In this case however, the impedance stays within normal range (for an LV lead) and stays stable at the new value, with no problems in capture threshold and no clinical symptoms. This is can be explained by a change in the LV pacing vector. Lead-related events (dislodgement, insulation breach, conductor fracture, fibrosis) evolve either gradually or erratically, and they often disturb the capture threshold (and the sensed signal). The pattern seen here is the fingerprint of a pacing vector reprogramming between two follow-ups: each LV electrode combination has its own electrode surface area and its own path through the myocardium, and therefore its own impedance.
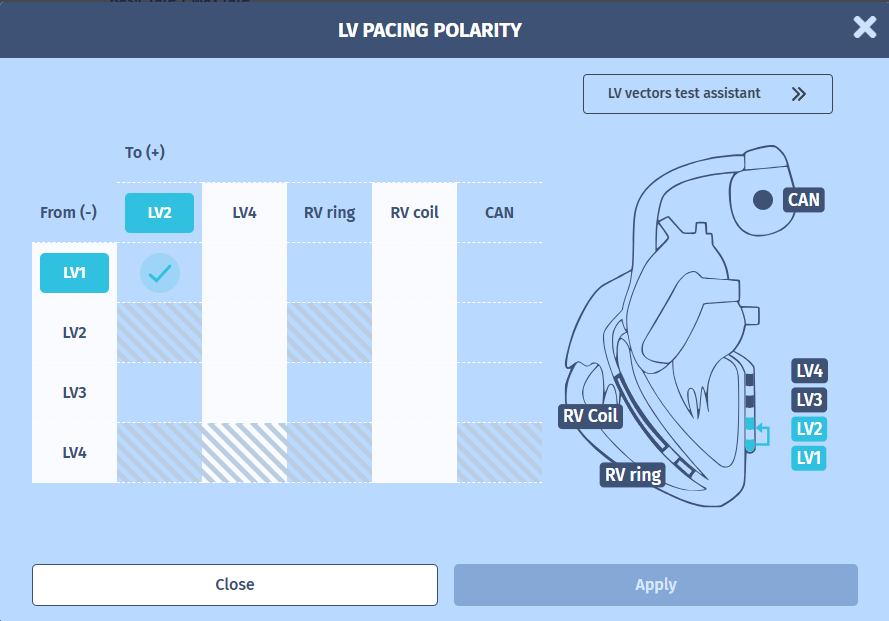
Here the current vector (LV1 – LV2):
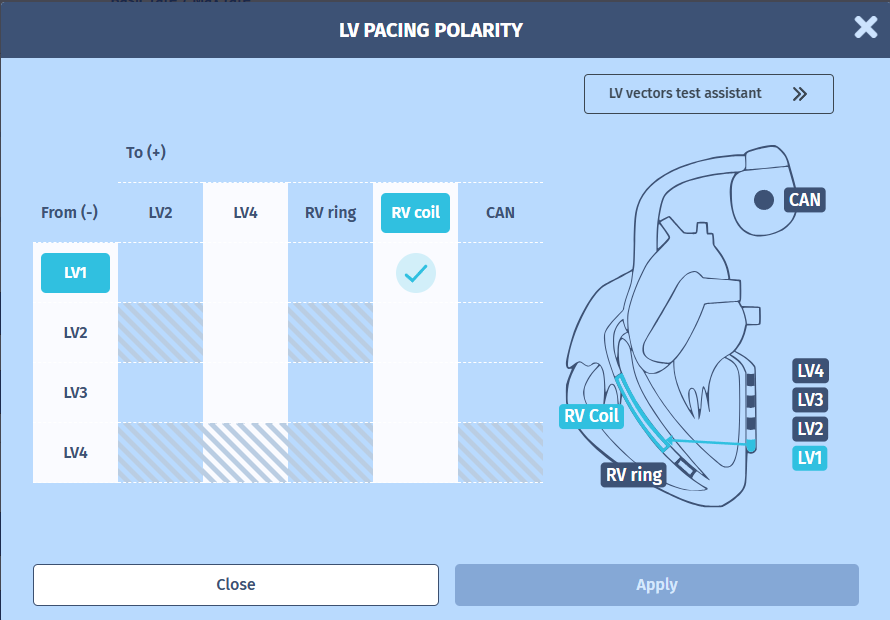
Here the previous programmed vector (LV1 – RV coil):
Why was the vector changed?
Two common reasons justify moving away from an LV → RV coil vector:
- A better LV capture threshold on an alternative vector; not the case here, thresholds were similar.
- Anodal capture on the RV coil; the reason in this patient.
At the previous visit, LV-only pacing in the LV1 → RV coil configuration produced a paced QRS with LBBB-like morphology, negative concordance in the precordial leads, and no R wave in V1, the ECG signature of pure right ventricular pacing. Despite the “LV” label of the pacing vector, the myocardium was being captured at the RV coil (anode), not at the LV1 electrode (cathode). This is anodal capture: the current density at the coil–myocardium interface is enough to depolarise adjacent RV tissue, and when the anodal RV threshold is lower than the cathodal LV threshold, the paced beat is RV-only.
Reprogramming to LV1 → LV2 removed the RV coil from the pacing circuit. Anodal capture on a small LV ring is anatomically and electrically implausible, so the paced beat now genuinely originates from LV1. The follow-up ECG confirmed this: positive R wave in V1 (RBBB-like pattern), reflecting the expected right-to-left activation wavefront from the postero-lateral LV site.
Take-home messages
- An abrupt, single-step, stable change on an impedance trend — without threshold or sensing changes — points to a vector reprogramming, not a lead problem. Always check the pacing configuration between the two follow-ups (possible on remote monitoring) before ordering imaging or planning revision.
- Any LV vector with the RV coil (or RV ring) as anode is vulnerable to anodal capture. Suspect it whenever the paced QRS morphology does not match the expected LV pacing site.
- Confirm true LV capture on the surface ECG: typically with an R wave in V1.
- 1
- Current
- Review / Skip
- Answered
- Exact
- Inexact
-
Question 1 sur 1
1. Question
ExactInexact